17 YEARS OLD FEMALE WITH LOOSE STOOLS AND VOMITING SINCE 1 WEEK.
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
CASE:-
17 year old female complaining of loose stools and vomiting since 1 week.
CHIEF COMPLAINTS:-
•loose stools since 1 week
•vomiting since 1 week
•fever since 3 days.
HISTORY OF PRESENTING ILLNESS:-
Patient was apparently asymptomatic One week back,she had outside food followed by which she developed loose stools and vomitings.
Loose stools:- 4-5episodes, water in consistency, non foul smelling, no blood tinged.
Vomitings:- 4-5 episodes, non projectile, non bilious, contents include food particles,Which subsided on taking medication,
Fever was incidious in onset, associated with chills and rigor,which subsided on taking medication
10years back,patient's mother observed swelling over the neck 4*4cm approximately and was diagnosed with HYPOTHYROIDISM and was on TAB.THYROXINE 25mcg....
Patient has history of eating slate pencils since 4 years.(5-6 slate pencils per day)
3 years ago :- history of itching and was taken to hospital which subsided on taking medication.
Since 3months patient is observing irregular menses,followed by dysmenorrhea,with clots.
Patient also complained of generalised weakness since 1week
HISTORY OF PAST ILLNESS:-
☆ Known case of hypothyroidism since 10 years and is on TAB. Thyroxine 25mcg
☆not a Known case of Diabetes mellitus, hypertension, asthma , epilepsy.
PERSONAL HISTORY:-
Diet:- mixed( non veg 2 times weekly)
Appetite:- normal
Sleep:- adequate
Bowel and bladder movements:- Regular
Addictions :- no Addictions
Allergy:- present 3 years ago, but subsided on taking medication.
FAMILY HISTORY:-
mother was a Known case of hypothyroidism and was on Tab. Thyroxine 100 mcg
GENERAL EXAMINATION:-
Patient was conscious, coherent ,cooperative, well oriented to time , place and person.
Pallor:-++
• Hyperpigmentation dots present over the buccal mucosa in the oral cavity.
• knuckle pigmentation was present.
•Acanthosis Nigricans ++
Icterus:- absent
Cyanosis:-absent
Clubbing:-absent
Lymph nodes:- bilateral cervical and submandibular lymph nodes palpable.
VITAL SIGNS:-
BP:-supine:- 130/80 mmhg
Standing:- 120/60 mmhg
Pulse rate:- supine:- 88BPM
Standing:- 83 BPM
spo2:- 98%
Respiratory rate:- 18CPM
GRBS:- 98mg /dl
SYSTEMIC EXAMINATION:-
CVS:S1,S2 heard,no murmurs
RESPIRATORY SYSTEM:
Inspection: trachea central in position
Normal vesicular breath sounds heard
BAE ++
LOCAL EXAMINATION:
Inspection:swelling at the anterior part of the neck,does not move with protrusion of tongue and moves with deglutition
Palpation :- disseminated margins,nodular,
size:6*7cms
Percussion :-
Auscultation :- no bruits
ABDOMINAL EXAMINATION:
Inspection :- no scars
Palpation :- soft,non tender
Auscultation :- BOWEL SOUNDS HEARD
CNS EXAMINATION:
CRANIAL NERVES: INTACT
Power
Rt UL-5/5. Lt UL-5/5
Rt LL-5/5. Lt LL-5/5
Tone-
Rt UL -N,Lt UL-N
Rt LL-N,Lt LL-N
Reflexes:. RIGHT LEFT
Biceps. ++ ++
Triceps. ++ ++
Supinator. ++ ++
Knee. ++ ++
Ankle. ++ ++
Plantar:. Flexion Flexion
•SENSORY
crude touch N N
Pain N N
Temperature N N
Fine touch N N
Vibration Right Left
Upper limb. 15 sec 15 sec
Lower limb. 11 sec. 10sec
Tibia. 14 sec. 14sec
Toe. 15sec. 15sec
Finger nose co-ordination : +





INVESTIGATIONS:-
Haemogram:-

Serumiron:-
Ferritin levels:-

Phosphorus levels:-

Serum calcium:-
Ultrasound Neck:-


Chest xray:-

Peripheral smear:-
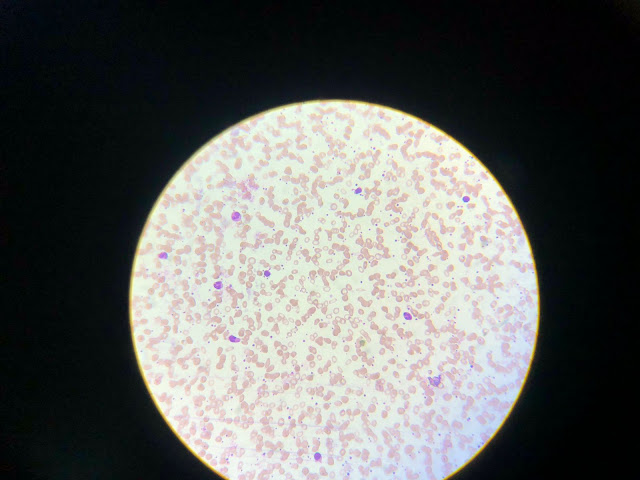
Diagnosis:- Dimorphic anemia.
ECG:-
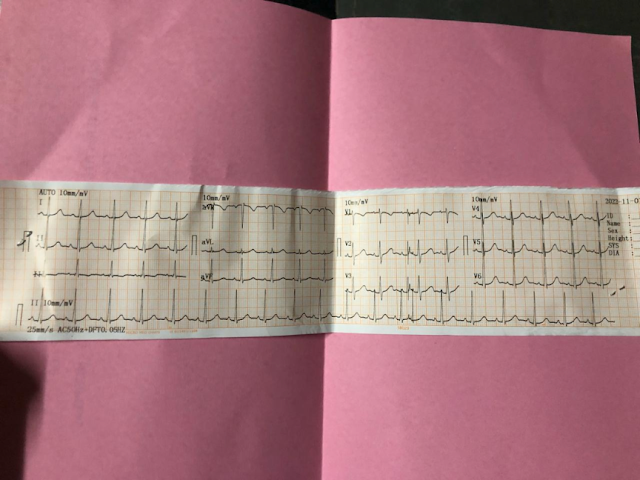


.jpg)
Comments
Post a Comment