A 51 year old male came with chief complaints of fever and cough since 5 days.
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment .
Vishal sarda
Roll no:-142.
A 51 year old male resident of idluru, farmer by occupation came to OPD at 2.00 pm on 4/1/22, with complaints of fever and cough since 5 days.
Chief complaints:-
• fever since 5 days
• cough since 5 days
• loss of appetite since 5 days
• burning micturition since 5 days
• body pains since 5 days.
History of presenting illness:-
•Patient was apparently asymptomatic 5 days back , then he developed fever which was intermittent , low grade , associated with chills and rigor, headache , periorbital pain .
Fever is generally low during daytime , but it increases during evening and night time .
So on 3/1/22 , patient went to a local RMP and took injections and dolo for fever.
Fever got relieved on taking medication but it again comes back.




•Patient also complains of burning micturition and decreased urine output since 5 days.
•Today in the morning he complained of Shortness of breath .
Past history:-
•Not a Known case of DM, HTN, asthma epilepsy, TB, CAD.
•H/O hydrocele surgery 20 yrs back.
Family history:- not significant.
Personal history:-
•Diet- mixed
•Appetite- reduced.
•Bowel movements- regular, bladder movements- reduced
•Sleep :-adequate
•Addictions:-drinks 1 beer on occasions.
Consumes toddy daily around 1 liter from the past 5 years.
•Allergies :- nil
General examination:-
•Patient is conscious, coherent , cooperative, well oriented to time ,place person, moderately built and moderately nourished.
•No signs of pallor, icterus, cyanosis, clubbing ,edema, lymphadenopathy.
Vitals :-
•Temperature :- afebrile
•BP :- 124 /80 mmhg
•Pulse rate :- 78/min
•Respiratory rate :- 16 cpm
•GRBS :- 275 mg /dl.
Systemic examination:-
•CVS :-S1, S2 heard, no murmurs.
•RS:- bilateral air entry present, normal vesicular breath sounds heard.
•Per abdomen:- soft, non tender.
•CNS:-
Higher mental functions :-normal
Reflexes:-
Right Left
Biceps :- ++ ++
Triceps :- ++ ++
Supinator:- ++ ++
Knee ;- ++ ++
Ankle:- ++ ++
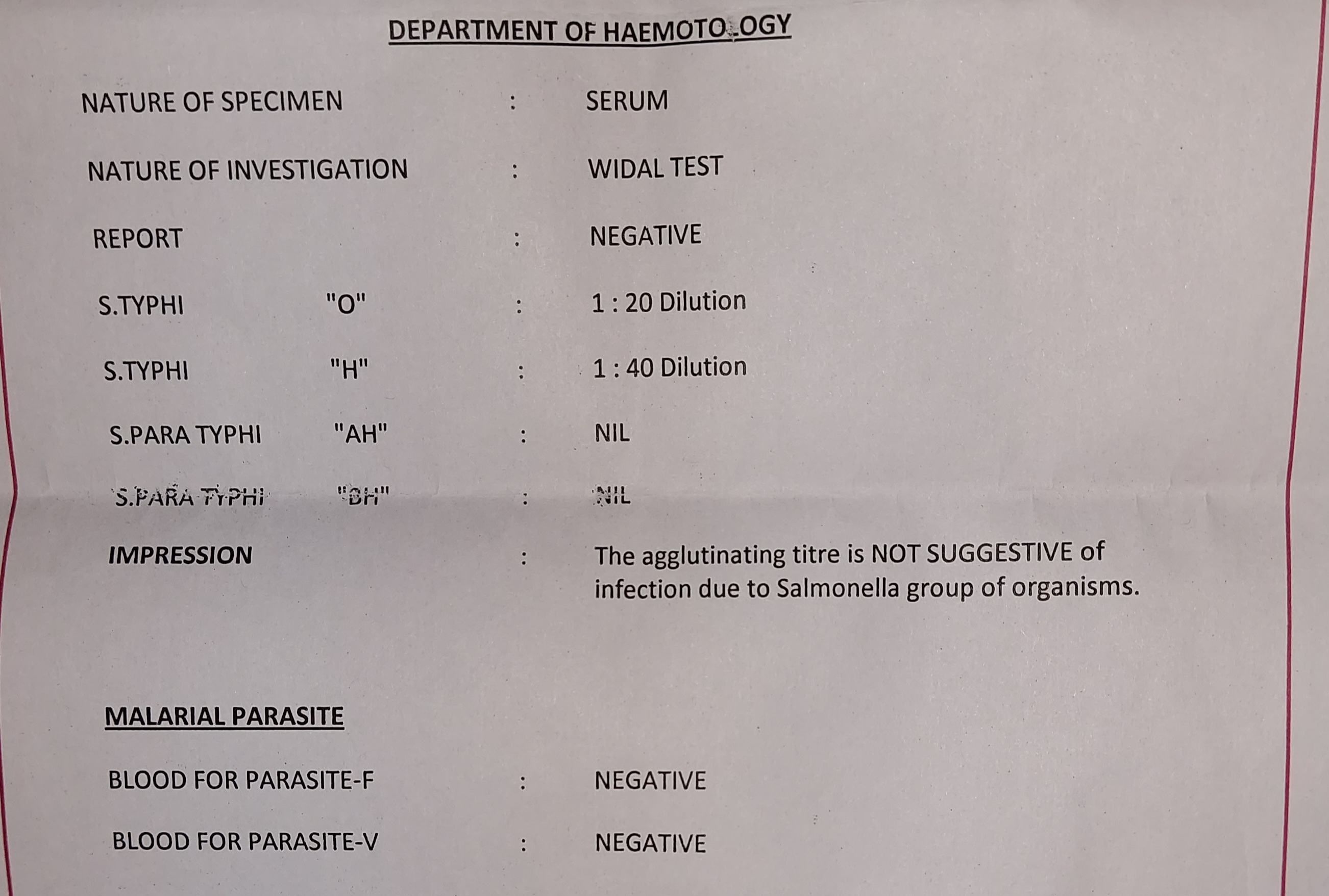
Investigations:-

On 4/1 /2023:-
Random blood sugar:-

HBsAg -RAPID:-


ECG:-



On 5/1/2023
HIV RAPID TEST:-










PROVISIONAL DIAGNOSIS:-
Viral pyrexia under evaluation with thrombocytopenia with polyserositis, ascites, AKI and denovo diabetes mellitus type 2.
Management :-
• nebulisation with salbutamol 4 respules iv
Stat
• IV fluids NS, RL @100ml/hr
• Tab.dolo 650mg PO/TID
• Inj. Neomol 1gm IV/SOS if Temp >101 F
• Inj. Optineuron 1 Amp in 100 ml NS PO/ OD
• Syrup citralka 10ml PO/OD
• Plenty of iv fluids
• strict I/O charting
• monitoring vitals 6th hrly
• Temperature charting 4th hrly.

.jpg)
Comments
Post a Comment